Chapter 2: Introduction to Anatomy - The Musculoskeletal System

Chapter 2: Introduction to Anatomy - The Musculoskeletal System
The Musculoskeletal System The structures forming the musculoskeletal system primarily provide support and mobility to the human body. To fulfill its function, it consists of numerous bones interconnected by joints and muscles that generate the necessary force for body movement. The histological foundation of the skeletal system is bone tissue. Bones, composed of bone tissue, are arranged in a specific manner, forming a complex and interconnected system. The joint system, encompassing every point of contact between skeletal elements, is highly variable, including numerous shapes, sizes, and functional capacities. Lastly and importantly, the muscular system acts as an engine for the above-mentioned systems, converting chemical energy into mechanical energy required for bodily movements.

Image by [kjpargeter](http://Image by kjpargeter on Freepik)
Bone Physiology
The musculoskeletal system comprises a large number of bones that are interconnected by joints and supported by over 600 muscles. Together, they form a skeleton with a central axis and four limbs. The variety of joint types ensures a broad range of motion, while muscles—layered and attached at different points on the bones—generate the forces necessary for movement. An adult human skeleton contains 206 individual bones, which are divided into two main regions:
- Axial Skeleton (80 bones): Includes the bones of the skull (both cranium and face), the vertebral column, the sternum, and the ribs. This central “axis” supports the head, neck, and trunk, and protects the brain, spinal cord, and thoracic organs.
- Appendicular Skeleton (126 bones): Comprised of the shoulder girdle (clavicle and scapula), the pelvic girdle (hip bones and sacrum), and the bones of the upper and lower limbs. These peripheral structures attach to the axial skeleton at the shoulder and hip joints, providing leverage and mobility for the arms and legs.
Together, the organization of bones, joints, and muscles allows for both stability and the diverse, coordinated movements essential to daily activities.

Image by [macrovector](http://Image by macrovector on Freepik)
Appendicular Articulation and Long Bone Structure
The appendicular skeleton connects to the axial skeleton to provide both support and mobility to the limbs:
- Shoulder Girdle: The clavicle (collarbone) and scapula (shoulder blade) form the shoulder girdle, which articulates with the bones of the upper limb at the shoulder joint. This mobile joint allows for a wide range of arm movements.
- Pelvic Girdle: The lumbar vertebrae and the sacrum combine to form the pelvis. The pelvis serves as a sturdy, basin-shaped support for the trunk and as the attachment point for the lower limbs. It transmits the weight of the torso to the legs and provides stability during standing and locomotion.
- Sexual Dimorphism in the Pelvis: There are marked differences between the male and female pelvis. In general, the male skeleton is larger and heavier. The female pelvis is wider and more circular in shape—an adaptation to accommodate childbirth.
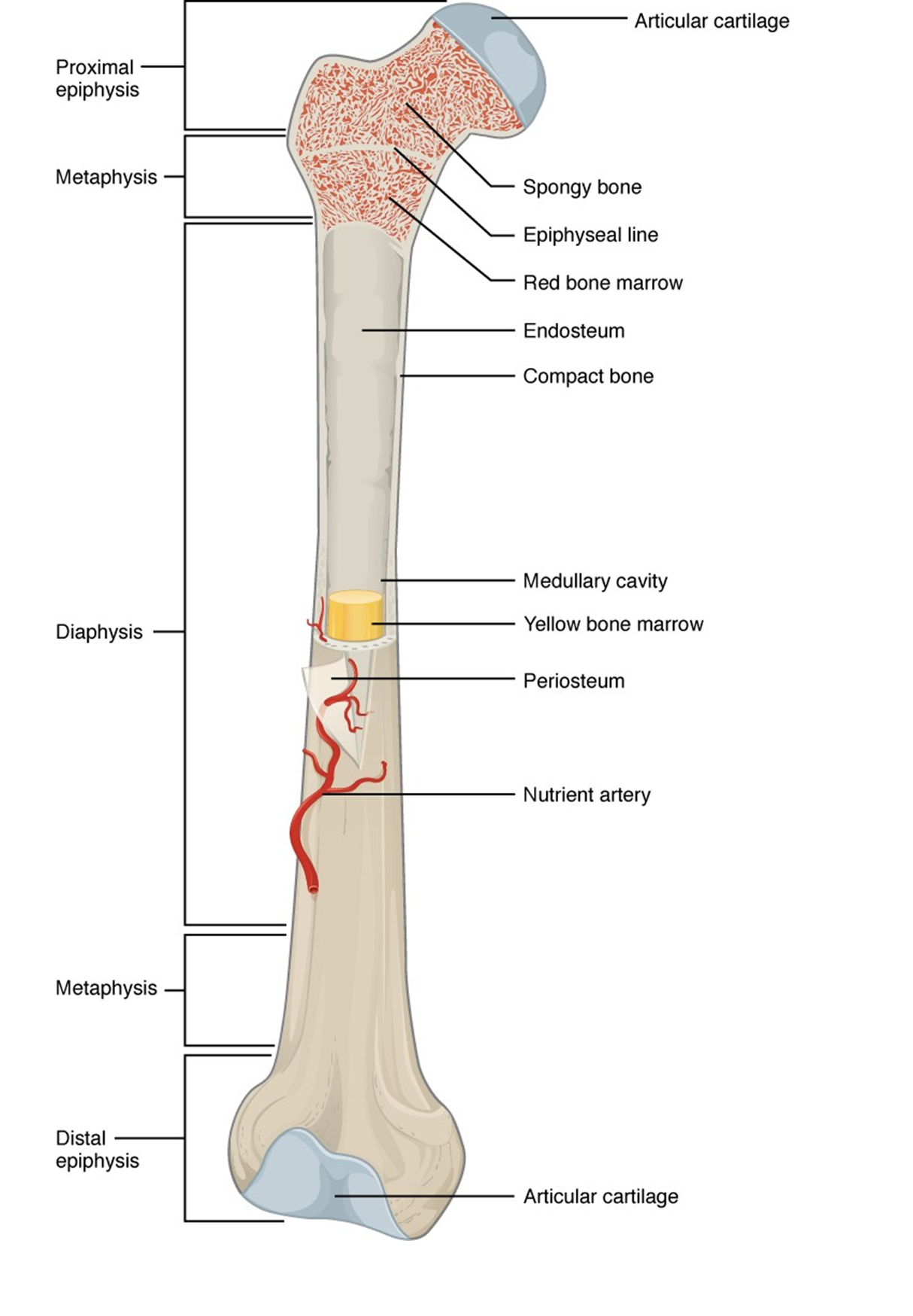
Long Bone Architecture
Long bones (such as the femur, humerus, and tibia) are composed of two forms of osseous tissue:
- Compact Bone:
- Arranged in cylindrical osteons (Haversian systems) that run parallel to the long axis of the bone.
- Provides strength and resistance to bending or torsional forces.
- Spongy (Cancellous) Bone:
- Located inside the ends of long bones (epiphyses), just beneath the compact layer and surrounding the medullary (marrow) cavity.
- Consists of a network of trabeculae (thin bony plates) that absorb shock and reduce overall bone weight while maintaining structural integrity.
Bone Cell Function and Remodeling
Bone is a living, dynamic tissue that undergoes continuous microscopic changes—growth, resorption, and remodeling—mediated by two principal cell types: osteoblasts and osteoclasts. Osteoblasts are small, highly active cells responsible for synthesizing and secreting the organic components of bone matrix, known collectively as osteoid. Within their abundant rough endoplasmic reticulum, mitochondria, and secretory vesicles, they produce collagen and other proteins that form the scaffold for mineral deposition. As they lay down osteoid, calcium and phosphate ions crystallize on this organic framework to create hardened, mineralized bone. Once osteoblasts finish depositing osteoid, most become inactive. A subset, however, becomes entrapped within the mineralized matrix in tiny cavities called lacunae, transforming into osteocytes. These mature bone cells maintain the surrounding matrix, sense mechanical strain, and help regulate mineral homeostasis. Osteoclasts are large, multinucleated cells derived from monocyte–macrophage lineages. They adhere tightly to bone surfaces—especially in small resorption pits called Howship’s lacunae—and secrete acids and lysosomal enzymes to dissolve mineral crystals and degrade organic matrix. This process, bone resorption, lowers local pH and allows decalcification and breakdown of collagen fibers. The balance between osteoid formation by osteoblasts (osteogenesis) and matrix breakdown by osteoclasts (osteolysis) depends on local mechanical and hormonal signals. Together, these opposing activities enable the skeleton to grow, repair microdamage, and adapt its architecture in response to changing loads.
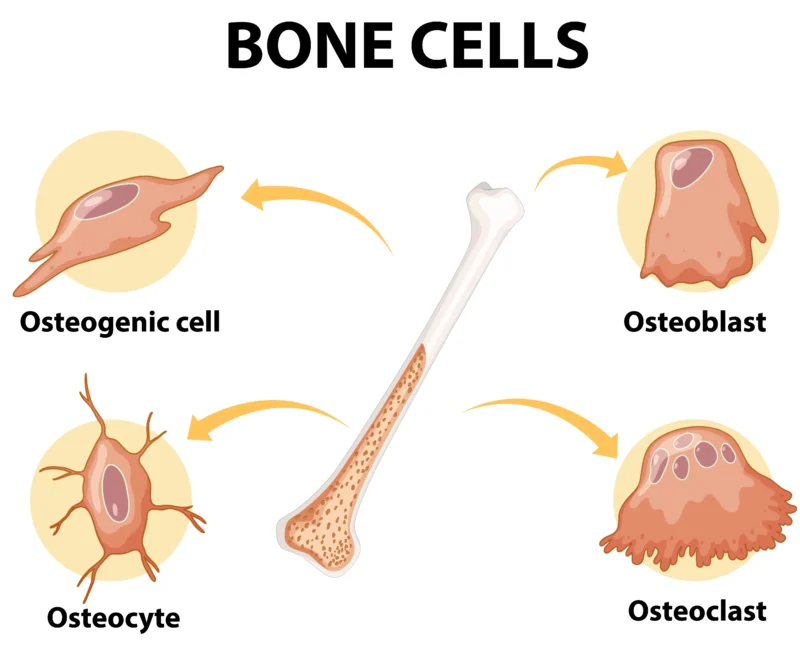
Image by [brgfx](http://Image by brgfx on Freepik)
Muscle Physiology
The human body contains over 600 skeletal muscles, accounting for approximately 50% of total body mass. Together with bones and subcutaneous fat, muscles define body shape. The arrangement of muscles, their relationships with each other, and their attachments to joints and bones determine voluntary body movements. Movement is the coordinated result of multiple muscles: as some contract, others relax.

Image by kjpargeter
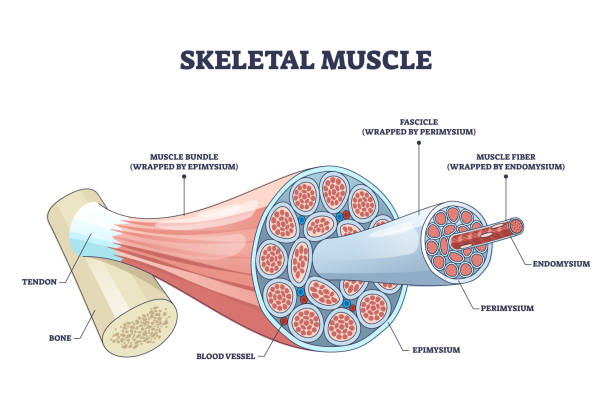
Organization of Skeletal Muscle
Skeletal muscles are organized with exceptional specialization to allow rapid contraction when stimulated and relaxation when the stimulus ends. The hierarchical structure includes:
- Muscle Belly enveloped by the epimysium.
- Fascicles (bundles of muscle fibers) wrapped in perimysium.
- Muscle Fibers (cells) surrounded by endomysium.
- Myofibrils within each fiber, composed of repeating units—sarcomeres.
- Myofilaments (thick and thin) within sarcomeres that drive contraction.
All components are bound by connective tissue layers (epimysium, perimysium, endomysium) that transmit force to tendons and bones.
Muscle Fiber Structure
- Length: 1–40 mm long, elongated and multinucleated.
- Sarcolemma: Plasma membrane of the fiber.
- Sarcoplasm: Cytoplasm containing abundant mitochondria and a specialized sarcoplasmic reticulum.
- Myofibrils: Hundreds to thousands per fiber, each made of parallel arrays of sarcomeres.

Sarcomere Anatomy
Sarcomeres are the functional contractile units, defined by Z-discs. They contain:
- Thin Filaments (Actin): Attached at Z-discs and extending toward the sarcomere center.
- Thick Filaments (Myosin): Central, do not attach to Z-discs, span the A-band of the sarcomere.
Bands and zones visible under microscopy change length during contraction:
- H-band: Region of only thick filaments, shortens during contraction.
- A-band: Length of thick filaments, remains constant.
- I-band: Region of only thin filaments, shortens.

Sliding Filament Mechanism
- Neural Signal: A motor neuron action potential reaches the neuromuscular junction.
- Neurotransmitter Release: Acetylcholine (ACh) released, binds nicotinic receptors on the sarcolemma.
- Action Potential Propagation: Travels along sarcolemma and T-tubules.
- Calcium Release: Sarcoplasmic reticulum releases Ca²⁺ into sarcoplasm.
- Cross-Bridge Formation: Ca²⁺ binds troponin, moving tropomyosin and exposing actin binding sites. Myosin heads attach, forming cross-bridges.
- Power Stroke: ATP hydrolysis energizes myosin, pulling actin filaments toward the center of the sarcomere, shortening sarcomere.
- Cross-Bridge Detachment: New ATP binds myosin, releasing the head and resetting it.
- Relaxation: Ca²⁺ is pumped back into the SR, tropomyosin re-covers binding sites, and the sarcomere returns to resting length.
Motor Units and Innervation
- Motor Unit: A single motor neuron and all the muscle fibers it innervates. It is the functional unit of skeletal muscle.
- Neuromuscular Junction: Specialized synapse where the motor neuron communicates with the muscle fiber’s motor endplate via ACh.
Molecular Players
- Actin & Myosin: Contractile proteins forming the cross-bridge.
- Troponin & Tropomyosin: Regulatory proteins controlling cross-bridge access.
- Calcium Ions (Ca²⁺): Trigger cross-bridge cycling.
- Adenosine Triphosphate (ATP): Provides energy for power strokes and cross-bridge release.
Together, these structural and molecular components enable precise control of muscle contraction and relaxation, essential for movement, posture, and metabolic functions.
Trunk Musculature and Vertebral Column
Posterior Trunk Muscles and Movement
The posterior muscles of the trunk play a key role in trunk mobility. Muscles such as the trapezius, teres major and minor, and latissimus dorsi work synergistically to coordinate movements of the trunk and upper limbs. The oblique abdominal muscles, together with the latissimus dorsi, facilitate trunk rotation.
Intermediate and Deep Trunk Muscles
Intermediate-level muscles, including the splenius capitis, splenius cervicis, and semispinalis, are responsible not only for rotating the head relative to the trunk but also act as accessory respiratory muscles. While all posterior trunk muscles share common actions, the deep muscles—particularly the erector spinae group—specialize in vertebral column movement, providing the wide range of flexion, extension, and lateral bending that characterizes spinal mobility.
Role in Respiration
Under normal resting conditions, prevertebral muscles are rarely active, as ventilation occurs without significant chest wall muscle involvement. However, during high respiratory demand, these deep muscles become vital accessory muscles of respiration.
Anatomy of the Vertebral Column
The vertebral column forms the vertical axis of the skeleton. It is a flexible structure composed of:
- 24 Vertebrae: Divided into cervical (7), thoracic (12), and lumbar (5) regions.
- Sacrum and Coccyx: Fused bones at the base of the column.
Intervertebral joints between vertebral bodies, including intervertebral discs and facet joints (formed by articular processes), allow the spine to move forward (flexion), backward (extension), and side-to-side (lateral flexion). Ligamentous support—such as the anterior and posterior longitudinal ligaments, interspinous and supraspinous ligaments, ligamenta flava, and intertransverse ligaments—ensures stability while permitting flexibility.
Spinal Curvatures
Viewed laterally, the spine exhibits four curves:
- Cervical Curve (7 cervical vertebrae)
- Thoracic Curve (12 thoracic vertebrae)
- Lumbar Curve (5 lumbar vertebrae)
- Sacral Curve (sacrum and coccyx)
These curves distribute mechanical stress during upright posture and movement.
Regional Vertebral Characteristics
- Cervical Vertebrae: Small bodies, bifid spinous processes (except C7), large triangular vertebral foramina, and transverse foramina for vertebral arteries.
- Thoracic Vertebrae: Larger bodies than cervical, costal facets for rib articulation on bodies and transverse processes, long sloping spinous processes.
- Lumbar Vertebrae: Massive bodies bearing greatest weight, short thick spinous processes, triangular vertebral foramina, and broad transverse processes.
Each vertebra articulates with its neighbors via intervertebral discs and facet joints, forming a sturdy yet flexible column that protects the spinal cord and transmits forces between the upper body and pelvis.
Upper Limb Anatomy and Articulations
Major Muscles of the Arm
- Anterior Compartment (Flexors):
- Biceps brachii and coracobrachialis lie superficially on the front of the arm.
- Function: Elbow flexion and supination of the forearm (biceps brachii); assists shoulder flexion (coracobrachialis).
- Posterior Compartment (Extensor):
- Triceps brachii covers the back of the arm.
- Function: Primary elbow extensor.
- Deep Arm Muscles:
- Brachialis (anterior) and anconeus (posterior) lie beneath superficial muscles, contributing to flexion and stabilization of the elbow.
Forearm Musculature
- Flexor Group (Anterior): Responsible for wrist and finger flexion; also contribute to forearm pronation.
- Extensor Group (Posterior): Responsible for wrist and finger extension; assist in forearm supination.
- Pronators and Supinators: Pronator teres and pronator quadratus mediate pronation; supinator and biceps brachii mediate supination.
Shoulder Joint Stability
A complex of ligaments, tendons, and muscles stabilizes the glenohumeral joint:
- Capsular Ligaments: Coracohumeral and glenohumeral ligaments thicken the fibrous capsule between the scapula and humerus.
- Coracoclavicular Ligament: Connects clavicle to scapula.
- Glenoid Labrum: A fibrocartilaginous rim that deepens the glenoid cavity, enhancing stability.
- Rotator Cuff Muscles: Supraspinatus, infraspinatus, teres minor, subscapularis — their tendons blend with the joint capsule to hold the humeral head in the glenoid fossa.
- Deltoid: Major abductor of the arm, reinforcing the joint capsule superiorly.

Elbow Joint and Associated Structures
- Articulations: Humeroulnar (trochlea to trochlear notch), humeroradial (capitulum to radial head), and proximal radioulnar joints.
- Collateral Ligaments: Ulnar (medial) and radial (lateral) collateral ligaments thicken the capsule on each side, preventing medial or lateral displacement.
- Movement: Hinge joint permitting flexion and extension; proximal radioulnar allows pronation and supination of the forearm.
Wrist and Hand Joints
- Distal Radioulnar Joint: Pivot joint enabling pronation and supination.
- Radiocarpal (Wrist) Joint: Condyloid articulation between radius and proximal carpal row; stabilized by palmar and dorsal radiocarpal ligaments and ulnar and radial collateral ligaments.
- Midcarpal Joints: Articulations between proximal and distal rows of carpal bones, permitting gliding movements.
- Carpometacarpal Joints: Especially the first carpometacarpal joint (thumb saddle joint) allows opposition.
- Metacarpophalangeal (MCP) Joints: Condyloid joints allowing flexion, extension, abduction, adduction, and limited circumduction of the fingers.
- Interphalangeal (IP) Joints: Hinge joints (proximal and distal phalanges) permitting flexion and extension.
Each of these articulations, reinforced by capsular membranes, ligaments, and surrounding muscles, ensures both the stability and the wide range of precise movements required for upper limb function.
Lower Limb Anatomy and Articulations
Superficial Muscles of the Lower Limb
Superficial muscles provide the primary force for lower limb movement:
- Quadriceps femoris: Powerful extensor of the knee; functions against gravity during standing and walking.
- Gastrocnemius: Plantarflexes the foot at the ankle and assists knee flexion.
- Adductor group (magnus, longus, brevis): Located on the medial thigh, they draw the limb toward the midline (adduction).
Intermediate and Deep Lower Limb Muscles
- Gluteal region: Includes gluteus medius and minimus, which stabilize the pelvis during gait.
- Thigh (posterior): Semitendinosus and semimembranosus, key hip extensors and knee flexors.
- Leg (posterior): Plantaris (with gastrocnemius) and soleus form the triceps surae, essential for standing and locomotion.
- Leg (anterior): Tibialis anterior and extensor digitorum longus mediate dorsiflexion and toe extension.
- Deep group: Includes gluteus minimus, the long and short heads of biceps femoris, popliteus, flexor digitorum longus, and flexor hallucis longus, critical for fine control and stabilization.
Hip Joint
- Stability: A strong fibrous capsule and ligaments (iliofemoral, ischiofemoral, pubofemoral) reinforce the hip, with the iliofemoral ligament forming an inverted “Y” and ranking among the body’s strongest.
- Articulation: Ball-and-socket joint between the femoral head and the acetabulum, deepened by the acetabular labrum.
- Movements: Flexion, extension, abduction, adduction, rotation, and circumduction.
Knee Joint
- Type: Hinge joint linking femur to tibia, bearing significant body weight.
- Stabilizers: Patellar ligament, anterior and posterior cruciate ligaments, medial and lateral collateral ligaments, and medial and lateral menisci.
- Articulation: Femoral condyles with tibial plateaus and patella gliding in the trochlear groove.
- Movements: Flexion and extension; menisci deepen articular surfaces and absorb shock.
Ankle Joint (Talocrural) and Foot Articulations
- Talocrural Joint: Hinge joint between tibia/fibula and talus; dorsiflexion and plantarflexion.
- Subtalar and Midtarsal Joints: Permit inversion and eversion.
- Tarsal and Metatarsal Joints: Include Chopart (midtarsal), Lisfranc (tarsometatarsal), and metatarsophalangeal joints, enabling complex foot motions.
- Ligamentous Support: Medial (deltoid) and lateral collateral ligaments stabilize the ankle; interosseous membrane binds tibia and fibula.
- Plantar Ligaments and Fascia: Maintain the arches of the foot and absorb load during stance.
Each muscle, ligament, and joint in the lower limb is specialized to combine stability with the flexibility necessary for upright posture, locomotion, and shock absorption during ambulation.
Topics in this lesson
🎓 Want to become a certified instructor?
This lesson is part of our FREE Calisthenics Instructor Certification course. Create a free account to track your progress and earn your certificate!